What is GM1 Gangliosidosis?
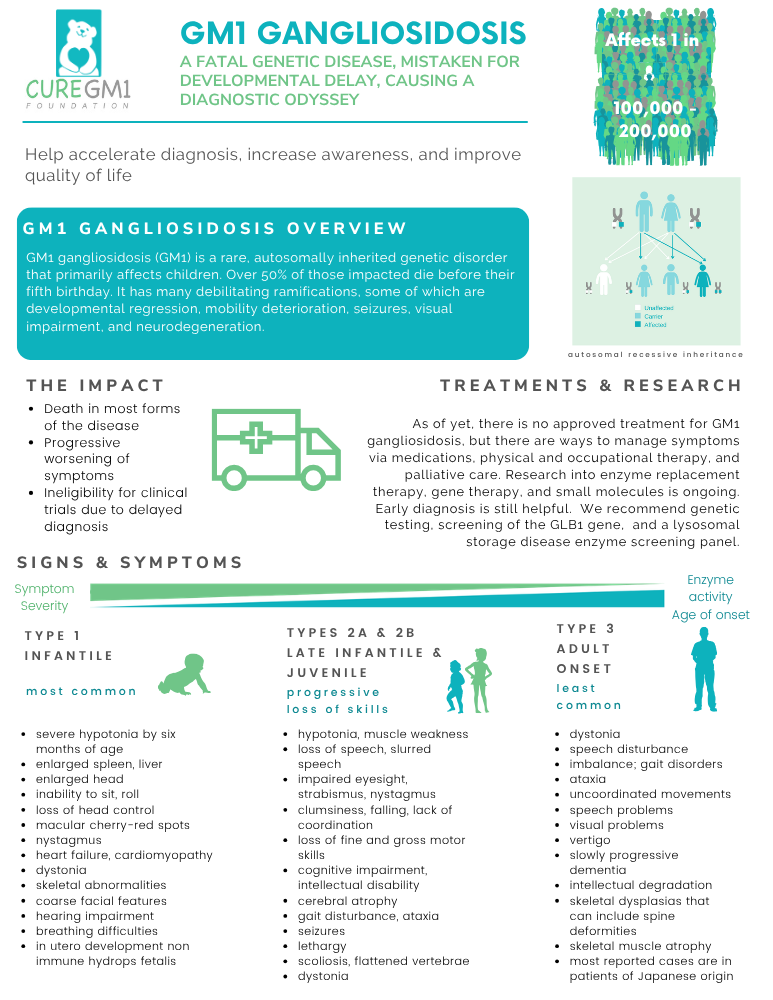
GM1 gangliosidosis is a rare, inherited lysosomal storage disease caused by mutations in the GLB1 gene. These mutations disrupt production of an enzyme called beta-galactosidase. Without enough of this enzyme, a fatty substance called GM1 ganglioside builds up in the brain and other organs, causing progressive neurological damage that cannot currently be reversed.
GM1 affects an estimated 1 in 100,000–200,000 newborns worldwide, making it one of the rarest childhood neurological conditions.[1,2] GM1 is autosomal recessive: a child is only affected if both parents each pass on a changed copy of the GLB1 gene.[3]
GM1 presents across three subtypes, with Type 2 divided into two subtypes based on age of onset. The subtypes differ significantly by onset of first symptoms, how quickly the disease progresses, and life expectancy.
There is currently no approved cure or disease-modifying therapy. Research into gene therapy, enzyme replacement therapy, and substrate reduction is actively underway. GM1 Clinical Trials Guide
Diagnosis is often delayed. Studies show the average time from first symptoms to a confirmed GM1 diagnosis can be months to years. Early symptoms overlap with other conditions, and most countries do not include GM1 on newborn screening panels. Raising awareness and expanding newborn screening are central to Cure GM1’s mission.
Learn about GM1
Download our overview of Gm1 gangliosidosis.
The Four GM1 Subtypes
Select one of the GM1 subtypes below to read the full clinical description, symptoms, and natural history.
GM1 Type 1
Infantile
Most common · 52.7% of cases in the curegm1.org/census.
The most severe form of the GM1 subtypes. Symptoms typically appear within the first 6 months of life, often following a period of apparently normal development. Affected infants experience rapid developmental regression losing skills they had acquired, along with progressive muscle weakness (hypotonia), seizures, loss of vision and hearing, and enlargement of the liver and spleen.
Distinctive early signs can include a cherry-red spot at the back of the eye (macula), coarsened facial features, and unusual skin markings (extensive Mongolian spots). Multi-organ involvement, including the heart, distinguishes Type 1 from later-onset subtypes.[4,5]
Life expectancy is typically 2–3 years. In some cases, Type 1 GM1 can be identified before birth (in utero).
Quick Facts:
• Onset: Birth to 6 months
• Survival: ~2 to 3 years
• Organ involvement: Yes
• Cherry-red spot: Often present
GM1 Type 1 subtype page
GM1 Type 2a
Late Infantile
18.8% of cases in the curegm1.org/census.
Children with Type 2a develop normally at first, then begin to show signs of regression between approximately 7 months and 2 years of age. Motor skills are typically affected first. Children may lose the ability to walk, sit independently, or use their hands, followed by speech loss and swallowing difficulties.
Seizures are common and often begin before age 5, sometimes before diagnosis is confirmed. Unlike Type 1, significant organ enlargement is uncommon, and cherry-red spots are less frequently observed.[5,6]
Children with Type 2a typically survive into mid-childhood. The NIH 10-Year Prospective Natural History Study is a comprehensive data source for this subtype.[6]
Quick Facts:
• Onset: ~7 months to 2 years
• Survival: Mid-childhood
• Seizures: Yes, before age 5
• Organ involvement: Mild/Rare
GM1 Type 2a subtype page
GM1 Type 2b
Juvenile
26.1% of cases in the curegm1.org/census.
Children with Type 2b usually develop normally until approximately 3 to 5 years of age, when gradual neurological decline begins. The progression is slower than Types 1 and 2a. Early signs often include subtle changes in gait, balance, speech, and coordination, followed by motor regression and eventually loss of independent ambulation.
Seizures occur in this subtype but with a highly variable onset from as early as age 6 to as late as the mid-twenties.[6] Dystonia (involuntary muscle stiffening) becomes increasingly prominent over time. Organ enlargement and cherry-red spots are rare.
Many individuals with Type 2b survive into early adulthood, with the longest-surviving patients now informing a growing body of adult-care literature.
Quick Facts:
• Onset: ~3 to 5 years
• Survival: Early adulthood
• Seizures: Variable
• Organ involvement: Rare
GM1 Type 2b subtype page
GM1 Type 3
Adult / Chronic
Rarest form · 2.4% of cases in the curegm1.org/census.
Type 3 is the mildest and rarest form of GM1. Symptoms most often emerge during the teenage years or early adulthood, though onset varies widely. The two defining features are dystonia (progressive involuntary muscle contractions causing abnormal postures) and abnormalities of the spinal vertebrae (dysostosis multiplex of the spine).[7,8]
Intellectual function is generally preserved, and organ involvement is not typical. Seizures are uncommon. Life expectancy is variable and can extend well into adult life.
Type 3 is disproportionately represented in individuals of Japanese descent and is frequently misdiagnosed as Parkinson’s disease, spinocerebellar ataxia, or idiopathic dystonia — meaning the true prevalence is likely underestimated.[7,8]
Quick Facts:
• Onset: Teens to early adulthood
• Survival: Variable
• Dystonia: Prominent
• Often misdiagnosed
Quick-Reference Comparison of GM1 Subtypes
How the four subtypes compare across key clinical features. This overview is a guide. Individual presentations vary.
GM1 Type 1 / Infantile GM1
| Age at symptom onset | Birth to 6 months |
| Typical survival | ~2 to 3 years |
| Speed of progression | Rapid |
| Organ enlargement (liver, spleen) | Yes, common |
| Cherry-red spot (macula) | Often present |
| Seizures | Common (early) |
| Dystonia | Late feature |
| Coarse facial features | Yes, typical |
| Intellectual disability | Severe |
| % of all GM1 cases | ~60% |
| Notable population | Global; elevated in Southern Brazil & Malta |
GM1 Type 2a / Late-infantile GM1
| Age at symptom onset | ~7 months to 2 years |
| Typical survival | Mid-childhood |
| Speed of progression | Moderate |
| Organ enlargement (liver, spleen) | Mild or absent |
| Cherry-red spot (macula) | Uncommon |
| Seizures | Yes, by age 5 |
| Dystonia | Yes, progressive |
| Coarse facial features | Mild or absent |
| Intellectual disability | Progressive |
| % of all GM1 cases | ~15 to 20% |
| Notable population | Global |
GM1 Type 2b / Juvenile GM1
| Age at symptom onset | ~3 to 5 years |
| Typical survival | Early adulthood |
| Speed of progression | Slower |
| Organ enlargement (liver, spleen) | Rare |
| Cherry-red spot (macula) | Uncommon |
| Seizures | Variable onset |
| Dystonia | Yes, prominent |
| Coarse facial features | Absent |
| Intellectual disability | Progressive |
| % of all GM1 cases | ~20 to 25% |
| Notable population | Global |
GM1 Type 3 / Adult-onset GM1
| Age at symptom onset | Teens to early adulthood |
| Typical survival | Variable |
| Speed of progression | Slow |
| Organ enlargement (liver, spleen) | Not typical |
| Cherry-red spot (macula) | Absent |
| Seizures | Uncommon |
| Dystonia | Prominent |
| Coarse facial features | Absent |
| Intellectual disability | Generally preserved |
| % of all GM1 cases | ~5 to 10% |
| Notable population | Disproportionate in Japanese descent |
Sources: Lang et al. 2020[4]; Regier et al. 2016[5]; NIH 10-Year Prospective Study (Tifft & Regier) 2024[6]; Orphanet[7]; MedlinePlus Genetics[8]; CGM1-01 INTERACT Briefing Document 2026[9]
Research Is Advancing for All GM1 Subtypes
There is currently no approved treatment or cure for any form of GM1 gangliosidosis, but clinical research is making progress. Active research programs include:
- Enzyme replacement therapy (ERT): Cure GM1 is actively working to bring an ICV ERT program into clinical development.
- Gene therapy: An NIH-sponsored Phase 1/2 trial (NCT03952637) using AAV9 delivery of a working GLB1 gene is actively enrolling for Type 2. A first-in-human prenatal gene therapy trial opens at UCSF in 2026. ClinicalTrials.gov
- Substrate reduction therapy: Oral small-molecule agents that reduce GM1 ganglioside buildup are in clinical trials (NCT06120946). ClinicalTrials.gov




References
1. Nicoli ER, Annunziata I, d’Azzo A, Platt FM, Tifft CJ, Stepien KM. “GM1 Gangliosidosis: A Mini-Review.” Frontiers in Genetics. 2021;12:734878. DOI: 10.3389/fgene.2021.734878
2. Brunetti-Pierri N, Scaglia F. “GM1 Gangliosidosis: Review of Clinical, Molecular, and Therapeutic Aspects.” Molecular Genetics and Metabolism. 2008;94(4):391–396. https://doi.org/10.1016/j.ymgme.2008.04.012
3. GeneReviews: GLB1-Related Disorders. Regier DS, Tifft CJ. NCBI Bookshelf. NBK164500. Last reviewed 2022. https://www.ncbi.nlm.nih.gov/books/NBK164500/
4. Lang FM, Korner P, Harnett M, Karunakara A, Tifft CJ. “The natural history of Type 1 infantile GM1 gangliosidosis: A literature-based meta-analysis.” Molecular Genetics and Metabolism. 2020;129(3):228–235. doi:10.1016/j.ymgme.2019.12.012
5. Regier DS, Tifft CJ. “GLB1-Related Disorders.” In: Adam MP, et al., eds. GeneReviews. Seattle (WA): University of Washington; 2016. GeneReviews
6. Tifft CJ, Regier DS, et al. “GM1 Gangliosidosis Type II: Results of a 10-Year Prospective Study.” JAMA Neurology, 2024 (PMC11348282). https://doi.org/10.1101/2024.01.04.24300778
7. Orphanet. “GM1 Gangliosidosis Type 3.” Orphan disease database. Accessed May 2026. orpha.net
8. MedlinePlus Genetics. “GM1 gangliosidosis.” U.S. National Library of Medicine. Accessed May 2026. medlineplus.gov/genetics/condition/gm1-gangliosidosis
9. Uyama E, et al. “Type 3 GM1 gangliosidosis: characteristic MRI findings correlated with dystonia.” Acta Neurologica Scandinavica. 1992;86(6):609–615. PMID: 1336295
10. MedLink Neurology. “GM1 Gangliosidosis.” Available at: medlink.com/articles/gm1-gangliosidosis. Accessed May 2026. medlink.com
Published May 2026. Cure GM1 does not prescribe medications or treatments. This information is being shared for educational purposes and discussion with your doctors.Visit us at curegm1.org

“People are telling us there’s nothing we can do for our daughters, we’re not accepting that. There is something we can do and that is to raise awareness and raise funding for them and for others.”
Kylie Harrison, Cure GM1 Board Member
Donate to Cure GM1
Help us find effective treatments and therapies so those living with GM1 can live long full lives